Abstract
Introduction. Anxiety and fear of public speaking are some of the common complaints of students during their studies. The prevalence and consequences for psychological well-being make it possible to discuss the fear of public speaking in the context of pathopsychological changes that contribute to or are a variant of a social anxiety disorder. At the same time, constant anxiety and emotional distress can contribute to the development of other comorbid pathologies such as depressive disorder, other anxiety disorders, or substance abuse as a way of coping anxiety. The development and implementation of effective psychological/psychotherapeutic interventions for self-help and psychological support with using a virtual environment has already proven itself in dealing with specific phobias and other anxiety states and can be applied in preventative measures for social anxiety disorder among students.
Aim. Investigate the impact of psychoeducation based on CBT protocol with a one-session virtual exposure on the level of students' social anxiety before public speaking and the features of social interaction during education.
Methods. Social anxiety assessment using the Social Phobia Inventory (SPIN), and Social Phobia Rating Scale (SPRS), clinical semi-structured interview, observation, and assessment of changes in virtual exposure.
Results. Compared with the control group, there was a statistically significant decrease in all indicators on the SPIN (p <0.001) and SPRS (p <0.001) scales in the experimental group 1 month after virtual exposure. Decreases in social anxiety on the SPIN scale before the intervention and one month after were statistically different depending on belonging to the experimental group (F = 5.06, p = 0.035) and time (F = 5.46, p = 0.029), and significantly from a baseline level of social anxiety (F = 124.8, p = 0.000). The significance of changes in the experimental group as a whole on the SPIN scale is achieved by reducing the indicator in the subgroup with a high level of social anxiety, where statistical significance is significant p <0.001. Differences in changes in the level of social anxiety on the SPRS scale before the intervention and one month after, depending on belonging to the experimental group (F = 9.39, p = 0.006), time (F = 12.33, p = 0.002) and baseline level of social anxiety (F = 12.06, p = 0.000) are also significant. According to the SPRS method, a statistically significant decrease in the rate of exhaustion and overall restriction imposing social anxiety (p <0.001) was found in the experimental group and a statistically significant decrease in the using of part of strategies avoidance behaviors and the influence of typical unproductive beliefs (p <0.05, in accordance).
Conclusion. Using psychoeducation based on CBT protocol with a one-session virtual exposure has proven to be an effective way of reducing the fear of public speaking. After 1 month undergoing a psychoeducational session using virtual exposure, a significant decrease in the intensity of anxious feelings, the impact of unproductive beliefs, and changes in behavior that underpinned them were revealed. It was noted that the most significant effect was achieved in the subgroup of participants with high input levels of social anxiety and manifest traits corresponding to the criteria of social anxiety disorder. Such changes may be explained by the need and timeliness of providing psychological support to this category of participants. Given that our findings are incomplete, they require further research and expansion of the experimental base.
Background
Scientific research around the concept of "anxiety" is becoming more relevant every year. Anxiety is seen as a normal, emotional response to the possible threat, accompanied by autonomic and somatic manifestations. Evolutionary anxiety allows a person to prepare for and / or respond to changes in the environment: to prevent potential threat, encourage the search and specification of the object of the threat, activating neuroendocrine and behavioral responses to provide a resource to act or maintain homeostasis in case of escape.
Everyone feels a certain nervousness and fear when comes up against a situation of stress, but the mentioned mobilization of internal resources as an adaptive reaction is temporary. Over time, anxiety can cause uncomfortable and potentially debilitating psychological and physiological changes. Thus, the signs of anxiety, which are prolonged, irrational and inappropriate force of manifestations, that occur in the absence of stressful events or stimuli and therefore interfere with everyday activities are called Anxiety Disorders [26].
It is a well-known fact that the excessive anxiety may occur in social situations where there is no direct threat to human life. Thus, M. Burnley and colleagues note that approximately 85% of the general population feel anxious about public speaking [8]. Such experiences range from a feeling of general tension to a panic state or freezing. M. Tillfors mentions in her article that the prevalence of anxiety about social interaction, which can be qualified as the mental pathology due to the degree of significant psychological and social discomfort, is equal to 7-13% during life in Western society [29]. As a rule, public speaking becomes the main trigger of stress for those who have a social anxiety disorder [8, 21, 29]. When people suffering from social anxiety disorder find themselves in situations where they become the center of attention, they experience strong uncomfortable emotions, which are exacerbated by autonomic changes and reinforce the belief that the danger is real. Thus, most of the people suffering from social anxiety disorder try to avoid situations in which they have to speak or interact in public [8, 28, 30]. Avoidance does not provide an opportunity to gain an effective corrective experience and refute false beliefs that support anxiety. This in turn is accompanied by growing difficulties in professional and educational areas, reduces social activity, forms a certain dependence on special conditions and circumstances in which the individual might feel comfortable [1].
It should be noted that anxiety and fear that accompany people before public speaking or precede joint activities can be assessed as an important part of social phobia. And this thought isn’t new in the literature [7]. This disorder is widespread and a number of publications is devoted to it. However, despite this fact a number of researchers point at the polemical character of the dependence of the expressed fear of public speaking and social phobia [3, 29]. This issue has been repeatedly raised in analytical reviews of the scientific literature. For example, reviews that were conducted by independent groups led by J. N. Hook and D. P. Valentiner in 2002 and S.G. Hofmann in 2004, differ in opinion [15, 16]. The other reviews indicate the existence of two most common pathopsychological variants of this interaction: the first includes views on anxiety before public speaking and social interaction as a form of social phobia, the other describes these symptoms only as a part of the anxious personality traits that rarely reach the clinical level of social phobia [7; 8].
In our opinion, the relevance of this issue is also that anxiety before public speaking and communication with peers is one of the typical complaints of students about psycho-emotional discomfort, along with complaints about depression and sensitivity to stress [5]. According to L.Kant, the environment usually negatively assesses those who show their fear of public speaking and will not be able to form a positive impression due to confident gestures, pronunciation or other behavior [17]. Feelings of shame, fear of looking awkward or humiliated in front of peers make one want to run away from the speech, to avoid answering before the audience or participate in group activities, and sometimes to seek help when necessary [12]. Some students who feel anxious about public speaking or related activities express feelings of sadness because of obsessive thoughts that others are looking at them or they are the center of attention. Others believe that what they say does not worth paying attention to. In both cases, it is possible to observe both cognitive distortion of unfavorable assessment by the environment and the inability to process the experience from an adult position. Lack or unwillingness to accept objective feedback often coincides with students' desire to be “perfect” (better, more promising, etc.), and in turn increases anxiety due to subjective and imposed pressure on “expected perfection” with low self-esteem [1]. Obsessive fear and emotional stress concerning looking imperfect, helps to fixate on physical feeling as those that can be subjectively controlled. It should be noted that students pay more attention to physical symptoms: tremors, feeling of cold and weakness in the hands, excessive tension in the shoulders, uncertain voice, rapid heart rate, sweating, facial redness, dizziness and shortness of breath, abdominal discomfort. Attempts to control autonomic and physical manifestations usually fail, and the partial successes they achieve reinforce unproductive beliefs and anxiety about that it will be worse or harder next time. At the same time, in academic or professional life, there is a certain prejudice about a straight-line correlation of the abilities and success during oral communication of the individual. Thus, students may feel their own "weakness" in the effective expression of opinions and subjective cognitive decline (often manifested in difficulties in remembering specific knowledge or words that a person was going to say) and therefore expect that they will form a negative impression of their own cognitive abilities or skills [6, 11].
We believe that this problem is a common phenomenon among students in Ukraine. But thorough research on this phenomenon is poorly covered in Ukraine in contrast to the publications of foreign experts. According to a survey by C. Knappe and colleagues published in 2011, approximately 25% of students experience a perceivable fear of public speaking [2]. A team study led by C. McConnell (2009) mentioned that speaking or having to speak in front of a large number of people caused anxiety in 75% of students surveyed [2]. In our opinion, the fear to express one's opinions due to an insecurity or low self-esteem is a typical problem for most students. At the same time a constant concern about possible joint activities or the need to speak in front of a live audience, that is keeping from achieving the life goals, including education or career, may be an evidence of social maladjustment [25].
In our article, we consider the way in which the virtual exposure experience can reduce anxiety before public speaking due to an opportunity to gain a corrective experience in a safe way. The use of virtual exposure aimed to work through anxiety before public speaking is described and analyzed in the works of P.L. Andersson, A.W. Blöte, A. Miloff, P. Lindner, L. Rothbaum, M. North, B. Wiederhold and others [4, 7, 13, 18-20, 22-24].
Scientific studies discuss that the mechanism of action of virtual exposure is no different from in vivo exposure [4]. Given that the exposure includes the replacement of the habit (strategy) of avoidance, forcing clients to approach dangerous stimuli deliberately, it allows the body to experience the absence of a danger. Considering this, it is an important task to shift from the perception of the environment as dangerous in dealing with anxiety caused by social situations [2]. The experience of exposure reduces the activity of the amygdala, which affects the reactivity of the sympathetic nervous system to stress, creating conditions and opportunities to consciously correct behavior. Thus, neural networks of the prefrontal cortex are involved in the work, allowing active, rational and effective thinking to influence the understanding of the context, and as a result to integrate the experience as positive. That is why the anxiety experienced during the exposure decreases over time, and social anxiety as a personal trait under the influence of experience becomes adaptive.
A meta-analytical study of 30 randomized controlled trials (n = 1057) found a significant effect when using of virtual reality for a variety of anxiety and related disorders, including social anxiety disorder, compared with the control group (waiting list) (g = 0.90), the mean value compared to the placebo effect (g = 0.78) and the absence of significant differences with in vivo exposure (d = -0.07) [10]. Analyzing the results, the authors of the study note that when virtual exposure is available and desirable, it should be preferred to in vivo exposure.
Despite the promising results of these studies, virtual reality as a therapeutic tool has not become widespread yet among mental health professionals. P. Lindner points out that at the beginning of 2016, several custom virtual reality platforms have been created for the development and implementation of the exposure, which allows for the widespread implementation of self-help programs [19]. Articles for 2014 by R.Moldovan and for 2019 by P. Lindner state that the successful use of one session of a virtual exposure helps to reduce social anxiety or fear of public speaking [20, 23]. Providing that most of them are designed for working through the specific phobias, we believe that the virtual environment can be set flexibly to simulate the anxiety stimuli in order to handle the experience of social anxiety disorder or fear of public speaking in particular.
After a preliminary analysis of the literature, there were identified the existing limitations for the use of virtual reality in conducting an exposure of anxiety before public speaking or social interaction [2]:
1. Criteria for inclusion stipulate that fear of public speaking should be a major social fear and a specific subtype of social anxiety disorder, which also has limitations when working with people who have generalized forms of the disorder or do not have it.
2. Most studies in which respondents were identified as having an anxiety disorder, no systematic diagnosis of concomitant psychiatric comorbidity was used. The presence of comorbid mental pathology was attributed to the exclusion criteria.
3. The use of non-standardized programs to create and conduct an exposure of virtual reality shows that it is difficult to give a generalized assessment and to compare the results within different studies at present time.
4. Study participants noted that anxiety was higher during social communication with virtual reality than during in vivo communication. In this connection the relief of discomfort after exposure was more noticeable.
5. Ethnic and racial diversity, which has influenced the style of communication and social interaction, in the samples of a number of studies, according to their authors opinion, remains as an aspect of discussion.
Aim
To investigate the impact of CBT-based psychoeducation using a one-session virtual exposure on the level of social anxiety of students before a public speech and the nature of social interaction during training.
We see the prospect in using the results of this pilot study to build programs to prevent the development or exacerbation of social anxiety disorder among students.
Methods and procedures
The search previous studies related to the theme articles was made through PubMed, Medline, Web-of-Science, BIOSIS, Cochrane Library and ResearchGate by us. To review current research, we have used articles published no later than 10 years ago, and the students were the subjects of the study. The search was carried out by the following keywords: "social anxiety"; "social anxiety disorder"; "sociophobia"; "anxiety before public speaking"; "exposure"; "virtual exposure"; "public speaking anxiety"; "social anxiety disorder"; "social phobia"; “virtual reality exposure therapy”.
Participants
The research procedure, inclusion and exclusion of criteria at all stages and ethical aspects related to the organization and conduct of the study were discussed at a meeting of the Department of Clinical Psychology of the Ukrainian Catholic University.
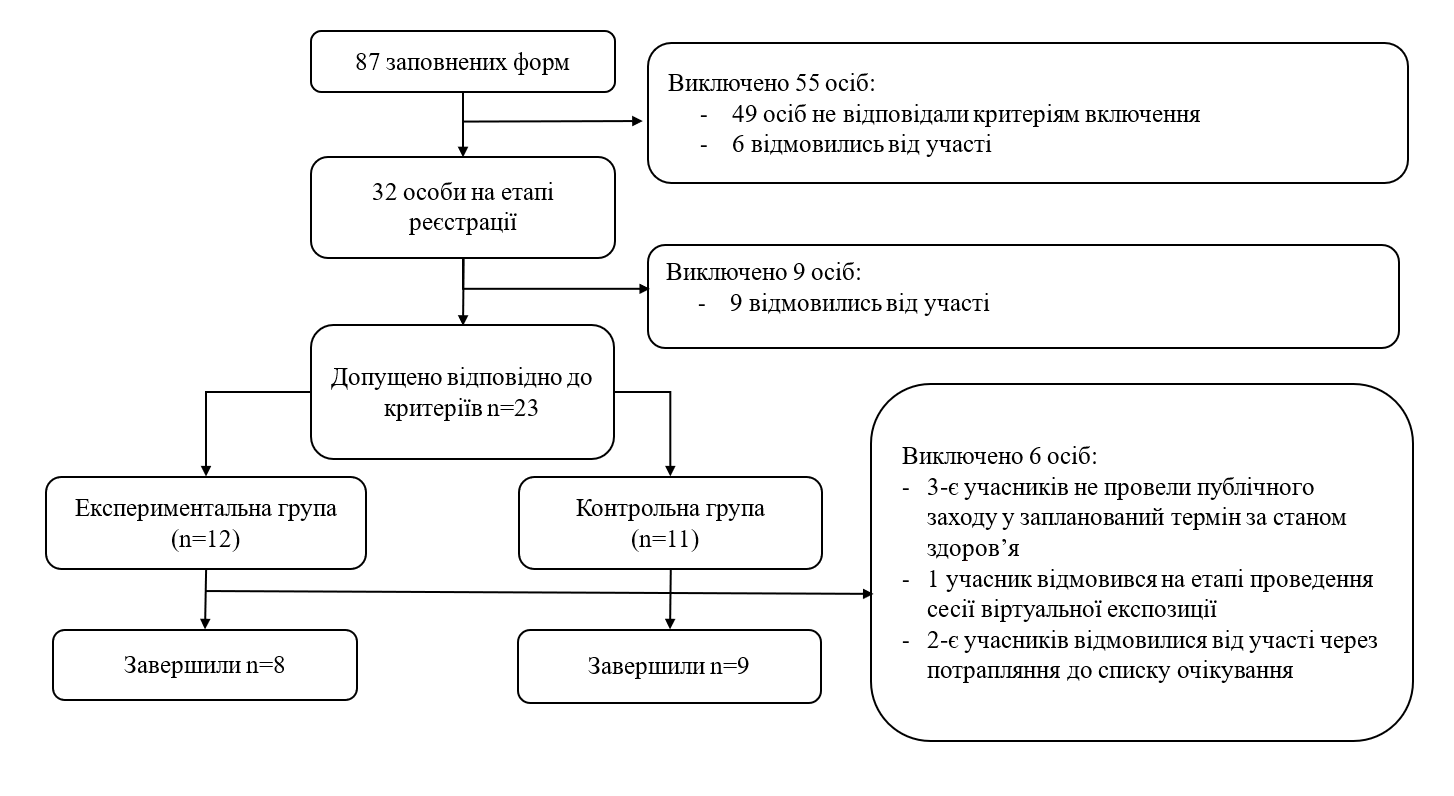
The search for the participants of the study was carried out among the students of the Ukrainian Catholic University, at the same time several participants were from other Higher educational institutions of Lviv. The total number of individuals who met the inclusion criteria was 23, 17 of them completed the pilot study (see Figure 1).
Figure 1. Sample Characteristics
The main inclusion criteria were: a) the age is over 18 years; b) to be a full-time student; c) to feel clinically significant psycho-emotional discomfort before public speeches or during joint educational activities subjectively; d) to give informed consent to the research and application of virtual reality. The exclusion criteria were: a) a psychotherapeutic treatment of social anxiety disorder during the last 6 months; b) a use of antidepressants or tranquilizers (other psychoactive substances) during the last 6 weeks; c) an absence in the anamnesis of psychotic episodes; d) the presence of problems with stereoscopic vision or problems with maintaining balance in previous experience of using virtual reality (all anamnestic data were collected only from the words of the participants).
Methods and assessment
To achieve the objectives of the study and to assess the level of social anxiety, the methods of assessing social phobia SPIN and SPRS translated by the Ukrainian Institute of CBT were used. Both methods have proven to be valid and reliable tools for assessing the level of social anxiety and its components [14,27]. The SPIN method is a scale of 17 questions in order to identify signs of social phobia. The evaluation is conducted for the last week and covers each of the areas of symptoms of social phobia: fear, avoidance strategies and physical symptoms. SPRS presents five rating scales that assess key components of social phobia: level of distress (exhaustion and limitations imposed by feelings of anxiety and intense fear), frequency of avoidance, elements of self-perception (shyness and awkwardness), use of protective behavior and typical negative beliefs. All these elements are used as targets for cognitive-behavioral therapy of social phobia or its individual elements.
Participants were also subjected to a semi-structured clinical interview to verify the symptom-complex according to the social phobia criteria in accordance with DSM-5, a participants-observation during exposure and subjective assessment scale (10-point rating scale) of anxiety level, feeling of duration of addressing anxiety and feeling of self-confidence (own competence).
Design of the study
At the pre-registration stage, the dissemination of information describing the objectives and design of the study through the internal e-mail of the university with the attached application form was used to search for participants who met the research criteria. The application contained information on personal data, place of study, consent to the planned public speech (to assess the effectiveness of the virtual exposure) and self-assessment of the level of anxiety before the public presentation on a scale from 0 to 10. Subsequently, in-personal clinical interview was conducted with all the participants who completed the form and indicated the subjective anxiety level equal to 7 and above. And they were suggested to complete SPIN and SPRS social anxiety self-assessment scales.
23 participants who met the inclusion criteria were admitted to the final stage (see Fig. 1). Given that this study was developed and conducted on a non-clinical sample of people with different levels of social anxiety we divided all participants before the formation of groups by level of social anxiety: low level of social anxiety - LSA (n = 7), medium - MSA (n = 10) and with a high level - HSA (n = 6). The distribution was based on the SPIN scale of social phobia with a range of 20-29 - mild, 30-39 - medium, 40 and more - high or severe levels of manifestations and on clinical interviews conduction. At the beginning of the study, we did not aim to form a clinical sample, but according to the results of the clinical interview, the study accepted participants who met the criteria for social anxiety disorder according to DSM-5. They formed 60% of the subgroup of the MSA and 100% subgroup of the HSA.
The pilot study was completed by 8 participants from the experimental group, all of them were girls (3 participants did not keep a public event within the established time limit due to the health problems and one participant refused at the stage of the virtual exposure session): еLSA = 3, еMSA = 3, еHSA = 2. 2 participants dropped out of the control group (both boys, who refused to participate due to getting into the control sample) and the distribution was as follows: cLSA = 3, cMSA = 3, cHSA = 3. The participants were interviewed repeatedly one month later after the study completion.
Description of interventions
In order to solve the research problems, we created a virtual environment with the help of 360-video. Several 360-video recordings with different plots were made. Each video contained different reactions and spatial positions of the listeners. And it was recorded in the different classrooms of the university. Students and teachers who acted as listeners were informed about the further use of the record and gave their consent.
The intervention program and procedure were based on the CBT-protocol for dealing with social phobia and its components. Before the exposition session, all participants were given a psychoeducational session on fear of public speaking and social phobia. In particular, it was highlighted how the range of automatic negative and catastrophic beliefs leads to changes in response at the physiological, emotional and behavioral levels. It was noted that avoidance and other coping strategies, which have been aimed at ensuring subjective security, lead to a deterioration in the effectiveness of activities (performance), inappropriate to the situation response, supported and cultivated irrational beliefs about themselves and the situation as a whole.
The next stage was a session with the use of virtual exposure: the total duration of the session was 40 minutes; the direct use of the virtual exposure lasted 3 minutes whereof. For a one-session virtual exposure, it was selected a video with audience of 13 listeners, who were sitting in three rows, and each participant individually demonstrated the behavior which was assigned according to the script. Participants were informed that if the experience of being in a virtual environment became unbearable, he / she could remove the helmet at any time during the exposure.
The exposure session began with a 15-minute introductory psychoeducation and functional analysis at the current time with an assessment of the level of anxiety. During the next 7-10 minutes of the session, the participant received information about the exposure technique, instructions for using virtual reality glasses and a plan of the session itself, which included three separate viewings of 360-videos in a virtual reality helmet. After each "minute" exposure, the participant rated own anxiety level from 0 to 10. The main focus of the first minute of the virtual exposure was the experience of virtual reality itself. After the first minute, the experimenter discussed with the participant the physical well-being to identify side effects of the virtual environment on the body, and the feeling of flooding and "authenticity" of the experience. Subsequently, the participant was asked to speak in front of a virtual audience. After the second and third "minute" exposures, the focus of the feedback was on specific stimuli that affected the participant's level of anxiety, thoughts, emotions, condition, and behavior. The third "minute" exposure was also performed after a preliminary measurement of the anxiety level.
After completion, it was discussed with the participant: whether personal condition had changed and how exactly, what are the hypotheses why it happened; what conclusions about personal reactions and the reactions of the audience were made. Throughout the virtual exposure, the experimenter observed the participant's behavior, noted with whom the participant spoke more (with the audience or with the experimenter), how this person moved and, thanks to the technical capabilities of the equipment, noticed where the participant's gaze had been directed. The observers recorded changes in behavior, level of anxiety and phrases of participants for further analysis.
Given that one of the criteria for inclusion was the willingness to hold a public speech live, participants additionally filled out a feedback form after the event. It assessed the level, duration and intensity of anxiety before a public speech, and other indicators that may have been affected by previous virtual exposure experience.
An identical psychoeducational meeting based on the CBT protocol without a virtual exposure was held for the control group. There was discussed the commitment to hold a public speech and to continue attending classes at the university throughout the experiment.
Limitations of the study
The organization and conduct of a pilot study using virtual reality set certain requirements for both us and the participants, and their compliance, in our opinion, could affect the results obtained. First of all, it concerns ensuring the procedure of exposure in a virtual environment: the technical equipment for the implementation of the virtual exposure belongs to the organizers, and to avoid copyright infringement, we have used only the virtual environment that was created by one of the organizers of the study.
Another challenge was the dissemination of information on research, search and selection of participants. As can be seen from the description of the study design, we were unable to gather a sufficient sample to enhance the capacities and ensure the purity of the experiment, and therefore this study was declared a pilot with the possibility of further continuation.
The inclusion criteria set for the purpose of the study imposed certain obligations on the participants (including the fact that during the experiment, participants should not seek other psychological help regarding social anxiety issues). Time spent on completing the documentation package and the requirements for planning and conducting a public speech, in our opinion, reduced the number of participants who completed the experiment and limited the dissemination of the results to the sampled population.
Results and discussion
A qualitative analysis of a previous study of participants of both the experimental and control groups (aged 18-25) found that most of them had recognized fear of criticism and fear to embarrass themselves as the main triggers for their social avoidance. At the same time the presence of "influential people or leaders" increased this likelihood and was identified as a modifying factor.
After the first minute of the exposure, a half of the participants in the experimental group noted that they focused only on a few participants from the audience, whose behavior had been demonstrative, contemptuous and they had kept to talk to each other all the time. We assume that the participant interprets such a reaction as dangerous, which causes stress reactions and makes stay focused on the potential threat only. And as a consequence, a subjective level of anxiety increases. It should be noted that a third of the experimental group could not remember who had been in the audience, the approximate number of people and other reactions of the audience, except for two people who had behaved demonstratively. It was also noticed that some of the participants could not focus on the task set to them due to a noticeable worry. And they continued to talk to the organizer of the study. Among other response options, they noted that they wanted to avoid eye contact with the audience and sometimes to laugh; commented that all this was unreal and in life they would not withstand such stress. We considered such responses as protective ones.
During the second minute, it was recorded that 6 of the 8 participants had not looked to the left-hand side of the audience, where the listeners had shown indifference. Participants could not remember what was happening in that part. The attention was again focused on the demonstrators. It increased the level of tension and irritability. This reaction is due to the previous experience and expectations of specific elements of the potential threat. Unlike the first minute of the virtual exposure, everyone completed the tasks of the exposure and was able to abstract one’s mind from the fact that the environment is virtual. At the same time, in the comments after the second minute of the exposure, the participants noted that they felt their own incompetence and defectiveness, which, in their opinion, were noticed by others (subjects of the virtual environment). The number of unconscious reactions increased markedly: adjusting of clothes or smoothing hair, redness, tension and squeezing of fingers, repeating a sentence or the last words several times, dry mouth, which interfered with speech. General complaints of chest discomfort, discomfort in the xiphoid process, mild dizziness and tension in the temples became more noticeable during reflection. All these changes were typical reactions for the participants of the experimental group in the life situations of public speeches, but were not provoked by the virtual environment. The data obtained during the second minute of the exposure made it possible to notice that the appeal to the protective behavior demonstrated at the beginning had decreased.
In the third part of the virtual exposure experiment, 75% of the participants felt the "peak of their own anxiety", but they completed the task without any signs of avoidance or other protective behavior. At the end of this minute of exposure, they all noted a significant decrease in anxiety (mean value did not exceed 4 points out of 10 maximum) and somatic discomfort during the exposure. There were noted orderliness of the behavior, reduction of autonomic reactions and confidence in the presentation of the material to the audience. 25% of participants showed a high level of anxiety, as during the previous stage. With their consent, it was decided to extend the exposure for the fourth minute. After the virtual exposure, the level of subjective anxiety before the public speech was low.
At the end of the exposure part, participants were asked to describe their own triggers and draw conclusions about how their thoughts, emotions, feelings, and behaviors changed under the influence of the exposure.
Comparative analysis showed a statistically significant difference in the t-test between the subjective level of anxiety (intensity and subjective discomfort, p<0.001) before the public speech prior to the virtual exposure and after it. Other indicators, such as "duration of anxiety" and "self-confidence", despite the participants' statements, did not have statistically significant differences.
For a month after the exposure, all participants of the experiment conducted control speech in front of a live audience (at the same time, they continued to attend classes at the university). After the control speech, the participants of the experimental group noted that they had significantly reduced anxiety connected with waiting for the event, it was easier for them to perceive the audience's reactions, the duration of anxiety and other discomfort from the beginning of the speech passed faster and was not as intense as before. The experience helped them to understand better personal reactions and to model behavior during the speech so as to reduce the impact of triggers. This added also a confidence.
Compared with the control group, there was a statistically significant decrease in all indicators on the SPIN (p <0.001) and SPRS (p <0.001) scales in the experimental group 1 month after the use of virtual exposure. The results of analysis of variance revealed that the decrease in the level of social anxiety on the SPIN scale before the intervention and 1 month after, statistically different in the experimental group compared with the control, depending on group membership (F = 5.06, p = 0.035), time (F = 5.46, p = 0.029), and significantly on baseline level of social anxiety (subgroups, F = 124.8, p = 0.000).
The mean scores and standard deviations of social anxiety levels for the subgroups of the experimental and control groups according to the preliminary assessment and monthly observation are given in Table 1.
| Baseline | Follow-up 1 month | ||||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| eLSA | 26,7 | 3,2 | 22 | 5,2 | -4,7 |
| eMSA | 33 | 2,6 | 29 | 1 | -4 |
| eHSA | 52 | 7,07 | 44,5 | 6,4 | -7,5 |
| cLSA | 27 | 2,6 | 26,7 | 2,5 | -0,3 |
| cMSA | 33,7 | 3,2 | 33 | 2,6 | -0,7 |
| cHSA | 52,3 | 4 | 51,7 | 4,2 | -0,6 |
Significance of changes in the experimental group in general on the SPIN scale is achieved by reducing the indicator in the subgroup with a high level of social anxiety, where the statistical significance is substantial p <0.001, while in the subgroups with primary low and medium level of social anxiety the changes are not statistically significant. Such results may indicate that the higher the level of social anxiety at the beginning is, the more noticeable the changes become after the application of psychoeducation based on the CPT protocol using a single-session virtual exposure.
A similar trend is observed in the case of analysis of the results obtained by the SPRS method. According to the results of analysis of variance, it was found that differences in changes in the level of social anxiety on the SPRS scale before the application of interventions and 1 month after were significant depending on membership in the experimental group (F = 9.39, p = 0.006), time (F = 12.33, p = 0.002) and baseline level of social anxiety (F = 12.06, p = 0.000).
The mean scores and standard deviations of the levels of social anxiety for the subgroups of the experimental and control groups according to the preliminary assessment and one-month observation are given in Table 2.
| Baseline | Follow-up 1 month | Difference | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Scale 1 | Scale 2 | Scale 3 | Scale 1 | Scale 2 | Scale 3 | Scale 1 | Scale 2 | Scale 3 | |
| eLSA | 5,3 (2,08) | 3,3 (1,5) | 4 (2) | 3,3 (0,6) | 2,3 (1,1) | 3 (1,5) | -2 | -1 | -1 |
| eMSA | 5,6 (0,6) | 4,6 (3,2) | 4,7 (2,5) | 3,3 (0,6) | 3,3 (2,08) | 3,3 (1,5) | -2,3 | -1,3 | -1,4 |
| eHSA | 6,5 (0,6) | 6,5 (2,1) | 6,5 (2,1) | 4,5 (0,7) | 5,5 (0,7) | 5,5 (0,7) | -2 | -1 | -1 |
| cLSA | 5,3 (1,1) | 3,3 (2,08) | 4,3 (1,5) | 4,7 (0,6) | 3,7 (1,5) | 4,6 (1,1) | -0,6 | +0,4 | +0,3 |
| cMSA | 5,7 (0,6) | 4,6 (0,6) | 4,7 (1,1) | 4,7 (0,6) | 5,3 (0,5) | 5 (1) | -1 | +0,7 | +0,3 |
| cHSA | 6 (0,6) | 7 (1,7) | 6,7 (1,1) | 6,3 (1,1) | 6,7 (1,5) | 6,3 (0,5) | +0,3 | -0,7 | -0,4 |
According to the SPRS method, the experimental group showed a statistically significant decrease in the rate of exhaustion and general limitation imposed by social anxiety (p <0.001). At the same time a decrease in the frequency of avoidance under the influence of social anxiety (scale 2: Frequency of avoidance) and changes in self-perception (scale 3: Feelings of shyness / awkwardness) during the study period are not statistically significant. Thus, the participants of the experimental group began to note that avoiding social situations did not bring them significant discomfort as it had been before the exposure.
It should be added that the SPRS methodology additionally allows to assess the severity of typical strategies for overcoming social anxiety, which the person resorts to (combined scale №4) and typical beliefs (confidence in them) that arise under the influence of social anxiety and reinforce it (combined scale №5). If 75% of the respondents in the experimental group avoided communication situations in the presence of others to address the feeling of anxiety, began speak a little (too generalized), but quickly, avoided eye contact with a partner in conversation and often focused on their hands before the exposure (SPRS results), then a month after the virtual exposure there was a statistically significant decrease in such behavior (data on a scale of №4 for these strategies, statistically significant at p <0.05). There was also a decrease in faith in such typical unproductive beliefs (from the list of the scale №5 of the SPRS method) as: "Everyone will notice my anxiety", "I will not be able to speak (support the conversation)" and "I lose control" (p <0.05).
Analyzing changes in specific elements of behavior and thinking and supplementing them with interview data a month after the exposure, we noted the following: all students in the experimental group noted that they were less likely to avoid planned public speaking or pre-arranged interaction with classmates (such as preparation of group projects or training in intervision groups). But other spontaneous activities still caused typical anxieties, desire to avoid and thoughts of their own incompetence.
Conclusion
The use of CPT-based psychoeducation using a one-session virtual exposure has proven to be an effective way to reduce fear of public speaking. One month after the psychoeducational session with the use of virtual exposure, there were found out a significant decrease in the intensity of anxiety, the impact of unproductive beliefs and changes in restrictive behavior that had reinforced them. Witnessing the reduction of psychological stress and exhaustion during joint activities, students began to show a willingness to implement the experience in life situations. It was noted that the most significant effect was achieved in a subgroup of participants with a high entry level of social anxiety, and manifest signs corresponding to the criteria of social anxiety disorder. Such changes are due to the need and timeliness of providing psychological support to this category of participants.
The results also suggest that the application of psychoeducation to social anxiety with virtual exposure can be used in the context of providing psychological support in the student environment, and we anticipate that it may be no less effective than in vivo exposure. The obtained positive results a month after the virtual exposure in the experimental group indicate that the use of such interventions can be promising to achieve a long-term effect and prevent negative consequences. Given that there were no statistically significant changes in the overall frequency of avoiding social interaction during other learning activities (other than planned activities) and in feelings of shyness, we believe that the proposed strategy of psychological support proved to be only as an element of emotional stabilization, and participants may need additional psychotherapeutic sessions.
However, our results are not complete and require further research and expansion of the experimental base, in particular, the duration of the effect after 3 and 12 months. And the study of the impact of interactive virtual environment on reducing social anxiety as an element of choosing the self-care interventions is also required. As a separate item, we set ourselves the task to make a try to investigate and describe why some participants with a high level of social anxiety tend to avoid social interaction when the intensity of social anxiety, exhaustion and social limitations due to it reduce.
Additional information
Conflicts of interest
The authors declare that they have no conflicts of interest to declare.
References
- Avramchuk O. Social anxiety disorder: relevance and perspectives. Psychosomatic Medicine and General Practice. 2018;3(3). doi:https://doi.org/10.26766/pmgp.v3i3.103
- Avramchuk O. Virtual exposure as an instrument to overcome student’s fear of public speaking and social interactions. Psychol J. 2020;6(1):9-17. doi:https://doi.org/10.31108/1.2020.6.1
- Allen M, Hunter J, Donohue W. Meta-Analysis of Self-Report Data on the Effectiveness of Public Speaking Anxiety Treatment Techniques. Commun Educ. 1998;38(1):54-77. doi:https://doi.org/10.1080/03634528909378740
- Anderson P, Price M, Edwards S, et al. Virtual reality exposure therapy for social anxiety disorder: A randomized controlled trial. J Consult Clin Psychol. 2013;81(5):751-60. doi:https://doi.org/10.1037/a0033559
- Bayram N, Bilgel N. The prevalence and socio-demographic correlations of depression, anxiety and stress among a group of university students. Soc Psychiatry Psychiatr Epidemiol. 2008;43(8):667-72. doi:https://doi.org/10.1007/s00127-008-0345-x
- Bodie G. A Racing Heart, Rattling Knees, and Ruminative Thoughts: Defining, Explaining, and Treating Public Speaking Anxiety. Commun Educ. 2010;59(1):70-105. doi:https://doi.org/10.1080/03634520903443849
- Blöte A, Kint M, Miers A, Westenberg P. The relation between public speaking anxiety and social anxiety: A review. J Anxiety Disord. 2009;23(3):305-13. doi:https://doi.org/10.1016/j.janxdis.2008.11.007
- Bögels S, Alden L, Beidel D, et al. Social anxiety disorder: Questions and answers for the DSM-V. Depress Anxiety. 2010;27(2):168-89. doi:http://dx.doi.org/10.1002/da.20670
- Burnley M, Cross P, Spanos N. The effects of stress inoculation training and skills training on the treatment of speech anxiety. Imagination, Cognition and Personality. 1993;12(4):355-66. doi:https://doi.org/10.2190%2FN6TK-AR8Q-L4E9-0RJ0
- Carl E, Stein A, Levihn-Coon A, et al. Virtual reality exposure therapy for anxiety and related disorders: A meta-analysis of randomized controlled trials. J Anxiety Disord. 2019;61:27-36. doi:https://doi.org/10.1016/j.janxdis.2018.08.003
- Goberman A, Hughes S, Haydock T. Acoustic characteristics of public speaking: Anxiety and practice effects. Speech Commun. 2011;53(6):867-76. doi:https://doi.org/10.1016/j.specom.2011.02.005
- Hancock A, Stone M, Brundage S, Zeigler M. Public speaking attitudes: does curriculum make a difference. J Voice. 2010;24(3):302-7. doi:https://doi.org/10.1016/j.jvoice.2008.09.007
- Harris S, Kemmerling R, North M. Brief Virtual Reality Therapy for Public Speaking Anxiety. Cyberpsychology Behav. 2002;5(6):543-50. doi:https://doi.org/10.1089/109493102321018187
- Nordahl H, Wells A. Metacognitive Therapy for Social Anxiety Disorder: An A–B Replication Series Across Social Anxiety Subtypes. Front Psychol. 2018;9. doi:https://doi.org/10.3389/fpsyg.2018.00540
- Hofmann S, Heinrichs N, Moscovitch D. The nature of social phobia: Toward a new classification. Clin Psychol Rev. 2004;24(7):769-97. doi:https://doi.org/10.1016/j.cpr.2004.07.004
- Hook J, Valentiner D. Are specific and generalized social phobias qualitatively distinct. Clin Psychol Sci Pract. 2002;9(4):379-95. doi:https://psycnet.apa.org/doi/10.1093/clipsy/9.4.379
- Kant L. Public Speaking Anxiety. University of Tennessee; 2000.
- Kampmann I, Emmelkamp P, Hartanto D, Brinkman W, Zijlstra B, Morina N. Exposure to virtual social interactions in the treatment of social anxiety disorder: A randomized controlled trial. Behav Res Ther. 2016;77:147-56.
- Lindner P, Miloff A, Hamilton W, et al. Creating state of the art, next-generation virtual reality exposure therapies for anxiety disorders using consumer hardware platforms: Design considerations and future directions. Cogn Behav Ther. 2017;46(5):404-420. doi:https://doi.org/10.1080/16506073.2017.1280843
- Lindner P, Miloff A, Fagernäs S, et al. Therapist-led and self-led one-session virtual reality exposure therapy for public speaking anxiety with consumer hardware and software: A randomized controlled trial. J Anxiety Dis. 2019;61:45-54. doi:https://doi.org/10.1016/j.janxdis.2018.07.003
- Merikangas K, He J, Burstein M, et al. Lifetime prevalence of mental disorders in U. S adolescents: Results from the national comorbidity survey replication–adolescent supplement (NCS-A) J Am Acad Child Adolesc Psychiatry. 2010;49(10):980-9. doi:https://doi.org/10.1016/j.jaac.2010.05.017
- Miloff A, Lindner P, Hamilton W, Reuterskiöld L, Andersson G, Carlbring P. Single-session gamified virtual reality exposure therapy for spider phobia vs Traditional exposure therapy: Study protocol for a randomized controlled non-inferiority trial. Trials. 2016;17. doi:https://doi.org/10.1186/s13063-016-1171-1
- Moldovan R, David D. One session treatmet of cognitive and behavioral therapy and virtual reality for social and specific phobias, preliminary results from a randomized clinical trial. J Cogn Behav Psychot. 2014;14(1):67-83.
- Morina N, Brinkman W, Hartanto D, Kampmann I, Emmelkamp P. Social interactions in virtual reality exposure therapy: A proof-of-concept pilot study. Technol Health Care. 2015;23(5):581-9. doi:https://doi.org/10.3233/THC-151014
- Pertaub D, Slater M, Barker C. An Experiment on Public Speaking Anxiety in Response to Three Different Types of Virtual Audience. Presence Teleop Virt. 2002;11(1):68-78. doi:https://doi.org/10.1162/105474602317343668
- Shri R. Anxiety: Causes and Management. JBS. 2010;5(1):100-18.
- Söyler E, Gunaratne C, Akbaş M. Towards a Comprehensive Simulator for Public Speaking Anxiety Treatment in Advances in Applied Digital Human Modeling and Simulation. Springer; 2017. doi:https://doi.org/10.1007/978-3-319-41627-4_18
- Spence S, Rapee R. The etiology of social anxiety disorder: An evidence-based model. Behav Res Ther. 2016;86:50-67. doi:https://doi.org/10.1016/j.brat.2016.06.007
- Tillfors M, Carlbring P, Furmark T, et al. Treating university students with social phobia and public speaking fears: Internet delivered self-help with or without live group exposure sessions. Depress Anxiety. 2008;25(8):708-17. doi:https://doi.org/10.1002/da.20416
- Westenberg P, Drewes M, Goedhart A, Siebelink B, Treffers P. A developmental analysis of self-reported fears in late childhood through mid-adolescence: social-evaluative fears on the rise. J Child Psychol Psychiatry. 2004;45(3):481-95. doi:https://doi.org/10.1111/j.1469-7610.2004.00239.x