Abstract
Introduction. The HIV epidemic, which affects millions of people in eastern Europe, remains one of the most important unresolved health issues. A patient-oriented approach to HIV-infected people improves the quality of medical care, affects the reliability of statistics, streamlines the planning and adequacy of public funds. The issues of comorbidity of the pathology of the digestive system in HIV infection and the formation of adherence to effective antiretroviral therapy (ART) are becoming particularly relevant. As a result, the role of family medicine practice in the detection, treatment, and management of gastrointestinal diseases in HIV-infected patients in Ukraine is growing.
The purpose of the study: To study the role of general practitioners in family medicine in the examination and management of HIV-infected people with concomitant pathology of the digestive system.
Material and methods. A survey was conducted among 200 general practitioners of family medicine (GPFM) and 292 physicians - limited specialists of a number of health care facilities in Kyiv and various regions of Ukraine by dint of a questionnaire developed through an internet survey and paper-based.
Results and discussion. General practitioners of family medicine noted rather low participation in the monitoring of compliance and side effects of ART, as well as the management of concomitant pathology of the digestive system (DS) in HIV-infected patients. Most of the surveyed physicians noted the lack of clear algorithms for action in the development of clinical routes of HIV-infected patients with concomitant pathology of the DS and almost all respondents confirmed the feasibility of using in their current practice algorithms developed for such patients. The vast majority of GPFM didn’t fully know the ways of movement HIV-infected patients from diagnosis to a stable virological/immunological response and, thus, were not able to fully manage the concomitant pathology of DS. HIV-infected patients who underwent and reacted negatively to ART didn’t return to GPFM and therefore didn’t receive adequate, continuous, comprehensive, and coordinated medical care for various DS pathologies. Returning of HIV-infected patients from limited specialists to GPFM has been low, sporadic, which may explain the decline in the ability of GPFM’s to effectively monitor the clinical outcomes of treatment of DS pathology and ART therapy side effects.
Conclusion. Find out some of the problems on detection of DS pathology in HIV-infected people and further management tactics of such patients have been clarified. Due to the inconsistency and insufficient volume of screening for comorbid pathology of the DS organs in HIV-infected patients, many chronic pathologies remain undetected in the practice of GPFM. The presence of untreated comorbid diseases of the DS organs in HIV infection may be a risk factor for reduced effectiveness of ART in such patients. Therefore, special attention of family physicians should be paid to the timely detection, treatment, and monitoring of HIV diseases in HIV-infected patients. It is considered expedient to introduce clear algorithms of joint actions of GPFM and limited specialists involved in the management of HIV-infected patients with concomitant DS pathology.
Background
The HIV epidemic, which affects millions of people in Europe, especially in the east, remains one of the most important unresolved health issues. The vast majority of new cases of HIV infection (79%) were detected in 2018 in the eastern part of the European region and 16% - in the EU / EEA countries. The share of new cases of HIV infection registered in Ukraine in the general morbidity in the European Region of WHO and in its eastern part was 11% and 14%, respectively [1]. In Ukraine in 2019, there was approved a new Clinical Protocol for the use of antiretroviral drugs for the treatment and prevention of HIV infection [2]. The introduction of new approaches in treatment over the past 5 years has achieved tangible results. HIV care is provided by 439 ART sites, the number of which has increased by a third since 2017. The expansion of the network of institutions and organizations providing medical care to PLHIV has increased mainly due to the opening of new sites based on outpatient-polyclinic health care facilities [3].
Important factors influencing the mortality rate from HIV-related diseases are the timely diagnosis of HIV infection, early onset of ART, building the adherence to treatment and the availability of appropriate support. Due to the widespread use of effective antiretroviral therapy (ART) in recent years, most HIV-infected patients achieve almost normal life expectancy, and opportunistic diseases have become less common [4]. However, HIV infection increases the risk of diseases that traditionally have not been considered HIV-related, including cardiovascular disease, kidney disease, liver disease, and some cancers [5]. And ART can cause a variety of complications that reduce adherence to treatment and leads to the need for its replacement and even cancellation. Pathology of the digestive system and its impact on nutrition, immune status, etc. plays a significant prognostic role for the course of HIV infection. With its progression increases the share of liver and intestinal diseases [6,7]. The analysis of statistical data showed that in Ukraine during 2013-2015 the results of the examination for the presence of markers of hepatitis B virus (HBV) and hepatitis C virus (HCV) in people with a first-time diagnosis of HIV infection did not change significantly. But the level of HCV infection (5.8% –73.5%) among the population of HIV infection by injection exceeds the level of HCV infection among the general population (2–3%). The presence of HCV markers is a proxy indicator of parenteral interventions, including injecting drug use. It is important to note that the coverage of research on markers of HBV and HCV, STIs does not reach the appropriate level in most regions of Ukraine. Considering the cofactor effect of viral hepatitis, STIs on HIV transmission, suggest an increase in the complex medical, social and economic burden of these infections [8]. Knowing that the greatest difficulties arose in counseling the patients about preventive interventions related to care and treatment, the doctors must pay attention to comorbidities and preventive screening, compliance with the requirements of the clinical protocol before prescribing ART [9].
It should be noted that the current legal regulation of the organization of comprehensive medical care for people living with HIV is entrusted to the private counseling room "Dovira". It takes place with the involvement of other specialties physicians, other professionals and referring patients to relevant health care facilities, according to industry standards in the field of health care [10]. At the same time, the loss of a holistic approach to the patient reduces the quality of medical care, affects the reliability of statistics, leads to irrational planning and inadequate use of public funds [11].
With the experience in managing other chronic diseases, general practitioners (GPs) are also appropriate for monitoring and coordinating an interdisciplinary approach in the management of HIV-infected patients [12,13]. Thus, according to the results of surveys of GPs and infectious disease doctors, it was noted that GPs with extensive experience in HIV management provided quality care to these complex patients [13]. It is particularly important that it is family physicians who can reduce the so-called lost opportunities for early diagnosis of HIV. Which include timely contact with the health care system due to a clinical manifestation that may be caused by HIV. Or it often occurs in people with HIV-infection, but without a diagnosis of HIV for 30 days [14]. The importance of strengthening in-depth training of family physicians on the management of HIV patients and the need for ongoing training on modern guidelines, protocols, instructions on various issues of HIV infection is emphasized in the context of the high incidence of disease of HIV and other bloodborne infections [15,16].
In this regard, considering the growing role of primary care physicians, especially GPs, in the management of HIV-infected patients, especially in the event of comorbidities, there was conducted a survey of activity of physicians of various specialties in this area.
Aim
To investigate the role of family physicians in the examination and management of HIV-infected persons with concomitant pathology of the digestive system.
Methods and sample
A survey of doctors was conducted using a questionnaire, which we have developed by using a number of prototypes. This questionnaire was discussed and approved at a meeting of the sociological group of NMU named after O.O. Bogomolets. The surveys were conducted using paper media and online surveys among general practitioners-family phycisians and specialty physicians of a number of health care institutions in Kyiv and various regions of Ukraine. The questionnaire included sections with questions on diagnosing and managing HIV-infected patients, including those with concomitant pathology of the digestive system organs in the practice of physicians of various specialties. As well as identifying needs for additional training of physicians on the management of HIV-positive patients with concomitant pathology of the digestive system.
492 doctors took part in the survey, including 200 general practitioners (1 group) and 292 specialty physicians (2 group), which included doctors of other specialties, namely pediatricians, therapists, gastroenterologists, surgeons, anesthesiologists-reanimatologists, phthisiologists, obstetrician-gynaecologists, dentists, etc. A separate group of 53 infectious disease physicians (group 3) was identified, whereas these specialists are involved in the treatment and follow-up of HIV-infected patients in most cases directly. Statistical processing of the study results was performed using software in the package EZR 1.41 (Saitama Medical Center, Jichi Medical University, Japan).
Results and discussion
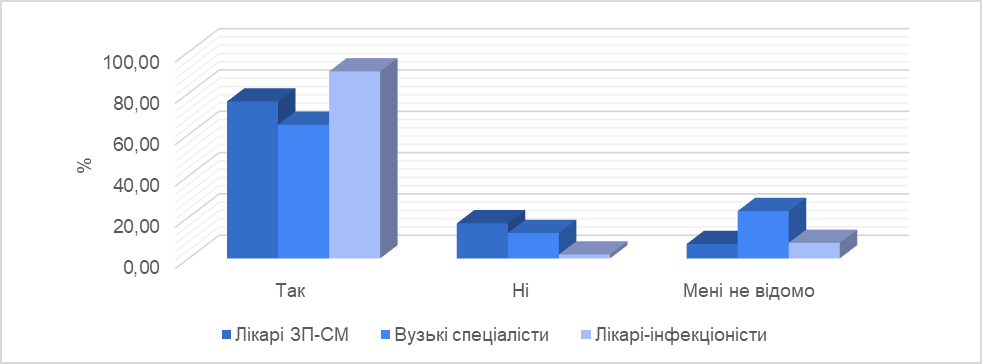
The analysis of the results of the survey of physicians showed that the presence of HIV-infected among their patients was noted by the majority (76%) of GPs, 64.7% of specialty physicians and 90.6% of infectious disease doctors. At the same time, 22.9% of specialty physicians and about 10% of GPs and infectious disease doctors stated that they were unaware of the presence of HIV infection in their patients (Figure 1).
Figure 1. Presence of HIV-infected patients in the interviewed doctors.
Most GPs (88.0%, p <0.05) consulted to and tested their patients for HIV (Figure 2), but only 31.0% of them offered screening to people at risk. 60.0% of GPs examined patients for clinical indications and only 9.0% of them examined contact persons. Whereas 100% of infectious disease doctors examined their patients for clinical indications. In the group of specialty physicians, 16.4% of doctors examined their patients from risk groups, 22.3% - according to clinical indications, 12.3% examined pregnant women, 40.4% of doctors examined to HIV the contact persons, and 8.6% of specialty physicians were not aware of specific categories of their patients for screening (Figure 2, Figure 3).
Figure 2. Conducting counseling and testing of patients for HIV infection.
Figure 3. Categories of patients who have been consulted to and tested for HIV by doctors.
At the same time, according to an analysis of suggestions of the surveyed physicians concerning improving physicians' personal medical practices in counteracting the spread of HIV, the decision of GPs to offer HIV screening to at-risk patients was more often their individually motivated choice.
The majority of GPs (73.0%) and specialty physicians (68.2%) reported that they had patients with chronic viral hepatitis B (CHB) in their practice. 72.0% of GPs and 64.4% of specialty physicians had chronic viral hepatitis C (CHC) patients, but 5.0% of GPs and 17.8% of specialty physicians were unaware of the presence of patients with CHB. And 6.0% of GPs and 20.9% of specialty physicians noted a lack of awareness about the presence of in them patients with chronic CHC.
It should be noted that 85.0% of GPs regularly offered HIV-infected patients counseling and testing for CHB and 90.0% for CHC, together with a general physical examination. But mostly only to those patients who sought primary care on their own. HIV-infected patients were offered counseling and testing for CHB by 59.9% and for CHC - 68.8% by specialty physicians. Whereas 100% of infectious disease doctors perform such a diagnosis. (Figure 4, Figure 5).
Figure 4. Counseling and testing for chronic hepatitis B.
Figure 5. Counseling and testing for chronic hepatitis C.
Along with this, the analysis of physicians' responses showed that only 39.0% of GPs and 37.3% of specialty physicians performed counseling and testing for CHB patients at risk. According to clinical indications, such a diagnosis was performed by more than half (55.0%) of GPs and 42.8% of specialty physicians.
Counseling and testing for CHC in patients at risk were performed by 36.0% of GPs, 30.14% of specialty physicians. As clinically indicated, the diagnosis of CHC was performed by 64.0% of GPs and 38.3% of specialty physicians. At the same time, 13.7% of GPs and 20.6% of specialty physicians were not aware of specific categories of patients for CHB and CHC screening.
When asked by doctors about the presence of HIV-infected patients with concomitant pathology of the digestive system, the majority of GPs (75.0%), specialty physicians (55.51%) and 100.0% of infectious disease doctors answered in the affirmative. However, 39.04% of specialty physicians were unaware of this (Figure 6).
Figure 6. Presence in doctors of HIV-infected patients with concomitant pathology of the digestive system.
Among the nosologies of digestive system diseases, which were more often diagnosed in HIV-infected patients, doctors noted CHC (67.50% of GPs, 35.85% of infectious disease doctors, 17.12% of specialty physicians), chronic pancreatitis (17.00% of GPs, 28.30% of infectious disease physicians), CHB (2.5% of GPs, 9.43% of infectious disease doctors, 13.12% of specialty physicians), gastric and duodenal ulcers (3.77% of physicians- infectious disease specialists, 10.27% of specialty physicians) (Figure 7).
Figure 7. Digestive system diseases that are more commonly diagnosed in HIV-infected patients.
GPs noted that in the outpatient stages of treatment in primary health care facilities, they (58.5% of responses) prescribed examinations to HIV-infected patients to detect pathology of the digestive system organs (gastroduodenitis, gastric ulcer and intestinal ulcer, cholecystitis, pancreatitis, hepatitis, etc.) or, according to their estimates, infectious disease doctors of the AIDS center (17.5%) or physicians of the AIDS centers / private counseling room "Dovira" (6.0%) or physicians / gastroenterologists of the CDC (5.5%). At the same time, 12.5% of GPs and 45.9% of specialty physicians found it difficult to answer this question. Meanwhile, only 7.5% of infectious disease physicians believed that such examinations were prescribed at the outpatient stages of treatment of HIV-positive patients by GPs, and about a third of infectious disease physicians (37.7%) noted the provision of such examinations by AIDS center physicians / private counseling room "Dovira" or physicians / gastroenterologists of CDC (Figure 8).
Figure 8. Appointment of examinations by doctors to detect pathology of the organs in the outpatient stages of medical care for HIV-infected patients in health care facilities.
Opinions of the interviewed doctors differed significantly on the issue of prescribing treatment and management of digestive system pathology (gastroduodenitis, gastric and duodenal ulcers, pancreatitis, etc.) in HIV-infected patients at the outpatient stages of their treatment. Thus, according to the answers of GPs, a significant part of them noted that such work was performed by GPs (59.0%), and only 3% and 16.0% of their answers indicated therapists of AIDS centres / private counseling room "Dovira" and therapists / gastroenterologists of CDC, respectively. About 10% of GPs found it difficult to answer this question.
At the same time, most infectious disease physicians (58.1%) and a third of specialty physicians (32.9%) found it difficult to answer this question. More than a third of infectious disease physicians identified physicians / gastroenterologists of CDC, and almost none of the infectious disease doctors noted the role of AIDS center physicians / private counseling room "Dovira" in prescribing treatment and management of digestive system pathology in HIV-infected patients in the outpatient stages of treatment. (Figure 9).
Figure 9. Prescribing treatment and management of digestive system pathology by doctors at the outpatient stages of medical care for HIV-infected patients in health care facilities.
Similar trends were observed in the analysis of responses of physicians of all groups to the question of monitoring compliance with treatment regimens for diseases of the digestive system in HIV-infected patients in the outpatient stages of care. When asked which doctor monitors adherence to such treatment regimens, most specialty physicians (47.7%), more than a third of GPs (35.9%) found it difficult to answer this important question. In 43.3% of the responses of GPs and 27.3% of specialty physicians, it was noted that the observance of such treatment regimens was monitored by GPs.
It should be noted that 44.4% of infectious disease physicians believed that it was the physicians of the AIDS Centers / private counseling room "Dovira" who controlled the treatment regimens of digestive system pathology in HIV-infected patients at the outpatient stages. Along with this almost none of them noted in the answers to the previous question the role of physicians-therapists of AIDS centers / private counseling room "Dovira" in prescribing treatment and management of pathology of the digestive system in HIV-infected patients in the outpatient stages of their treatment (Figure 10).
Figure 10. Monitoring the compliance of HIV-infected patients with the treatment regimens of the pathology of digestive system organs at the outpatient stages of medical care.
However, the detection of HIV infection and comorbidities, including the digestive system, is only the first step in the management of HIV-infected patients. According to the current legal regulations in Ukraine, the appointment of ART and monitoring of compliance with treatment regimens is carried out by AIDS centers. To implement effective management of HIV treatment and comorbidities, the routes for HIV-infected patients are developed in a number of health care facilities. This will allow them to be referred to a specialist, receive ART to achieve a stable virological, immunological and clinical response. Taking into account the importance of this area of activity, the awareness of doctors about the medical routes of HIV-infected patients was analyzed.
It was found that the majority of GPs (58.0%) did not fully know the routes of HIV-infected patients from diagnosis to a stable virological / immunological response and only 10.0% of GPs and 38.7% of doctors of groups of specialty physicians knew this, in contrast to the group of infectious disease doctors, who noted their sufficient awareness (71.7%) about the route of these patients (Figure 11).
Figure 11. Doctors' awareness of the further medical route of HIV-infected patients (from diagnosis to a stable virological / immunological response).
Regarding the questionnaire on the algorithms of action and routes of patients with concomitant digestive system pathology - the answers of doctors - narrow specialists showed a low level of awareness. The frequency of return of HIV-infected patients to GPs on the background of ART was analyzed. The frequency of counter-referrals of HIV-infected patients from specialty physicians to GPs for managing concomitant pathology, including the digestive system, was quite low, according to the responses of both GPs and specialty physicians.
According to the questionnaire, a very small number of GPs indicated that HIV-infected patients with various concomitant pathologies, including digestive organs returned to them from specialty physicians. Mostly those who had already achieved a stable virological response. Thus, 84 (41.2%) GPs believe that the return occurs in case of achieving SVR (stable virological response), 12 (5.9%) - during ART in case of occurrence or exacerbation of somatic diseases, 72 (35, 3%) - when they are on antiretroviral therapy (ART). 36 (17.7%) GPs found it difficult to answer the questions. Along with this, most GPs noted that patients who were on antiviral treatment or discontinued it for various reasons returned to them only in isolated cases.
In the estimations of surveyed GPs, this significantly reduced their ability to provide effective medical care to this category of HIV-infected patients with comorbidities, including the digestive system, in the current practice of family medicine. As well as to form a positive compliance to HIV-positive patients’ adherence with effective ART.
Among infectiologists, 52.8% believed that HIV-infected people returned to a GP in cases of ART discontinuation, and 47.2% found it difficult to answer. The vast majority of specialty physicians 154 (52.4%) could not answer this question (Figure 12).
Figure 12. Cases of reverse referrals of HIV-infected patients from specialists to GPs.
Regarding the issues on coordination of complex treatment, knowledge of all problems related to ART and concomitant pathology of digestive system in HIV-infected patients, the vast majority of physicians in all three groups believed that this function should be entrusted to GPs. At the same time, only 7.1% of GPs and 4.6% specialty physicians assigned this function to private counseling room "Dovira" (Figure 13).
Figure 13. Coordination of complex treatment of HIV-infected patients.
The opinions of physicians on the adequacy of medical care for HIV-infected patients and its impact on the effectiveness of treatment of HIV-infected patients were analyzed separately. Thus, the vast majority of physicians surveyed believed that existing medical supervision was insufficient, and this could affect the effectiveness of treatment. Herewith 45 (84.9%) infectious disease doctors suggested that insufficient medical supervision could significantly reduce it.
According to a survey of physicians, most GPs did not treat patients with CHB and CHC. Slightly more of this was done by specialty physicians and mostly by infectious disease doctors.
It should be noted that the vast majority of GPs (53.0%) did not know how to route HIV-infected patients from diagnosis to achieving a clinical result in full, 48.0% were able to partially and 5.0% did not know how to do it at all. Only 34.0% of GPs and 27.7% of specialty physicians knew it in full, in contrast to the group of infectious disease doctors, the vast majority of whom (67.9%) knew in full and in part (20.8%) this route of patients. On average, about 20.0% of physicians in groups 1 and 2 needed additional training (Figure 14).
Figure 14. Ability to route the HIV-infected patient from diagnosis to clinical outcome.
A similar situation in the responses of physicians of both groups was also observed for patients with CHC, CHB from diagnosis to clinical outcome.
According to the results of the questionnaire, the need for additional training of doctors on the management of HIV-positive patients with concomitant pathology of the digestive system was also identified. Thus, the majority of respondents stated that they had received additional training on HIV / AIDS, but at the same time, the vast majority of respondents noted the lack of their training on CHB and CHC infections.
When asked about the additional training on screening, diagnosis, treatment and integrated management of HIV-positive patients with concomitant pathology of the DS, the vast majority of surveyed physicians answered that such training was not provided (Figure 15):
Figure 15. Additional training on screening, diagnosis, treatment and integrated management of HIV-positive patients with concomitant pathology of the digestive system organs.
Most physicians noted the need for systematic additional training on HIV, CHB and CHC infections, as well as additional training on screening, diagnosis, treatment and integrated management of HIV-positive patients with concomitant pathology of the digestive system. What is more, they need it at a convenient distance education or in person-distance education in forms of thematic improvement cycles or short-term seminars or trainings.
In their comments to the questionnaire, about two-thirds of respondents said that they were more or less familiar with the legal documents on HIV in health care facilities at different levels of care. But most of them noted the lack of clear regulation and coordination their comprehensive interaction in cases of comorbid pathology in HIV-infected patients, including the digestive system.
Most GPs surveyed noted that they often encountered the side effects of antiretroviral therapy (ART) in HIV-infected patients. But noted a very low participation in monitoring ART compliance with such patients and the management of comorbidities, as well as monitoring for side effects.
Most of the interviewed physicians noted in their comments the lack of clear algorithms for developing clinical routes for HIV-infected patients with concomitant digestive system pathology, and almost all respondents confirmed the appropriateness of using management algorithms developed for such patients in their current practice.
Thus, our analysis of a survey of physicians on the diagnosis and management of HIV-infected patients with comorbidities of the digestive system showed the role of GPs in the current examination and management of HIV-infected people with comorbidities of the digestive system.
Conclusions
- The analysis of the results of the survey of physicians showed that the majority of general physicians examined their patients for HIV infection. The vast majority of them (75.0%) were informed about the presence of digestive system pathology in known cases of HIV-infected patients. 85.0% of GPs regularly offered HIV-infected patients counseling and testing for CHB and 90.0% for CHC, along with a general physical examination, but mostly only to those patients who sought primary care on their own.
- The majority of GPs (58.0%) did not fully know the routes of movement of HIV-infected patients from diagnosis to a stable virological / immunological response and thus did not have the opportunity to fully screen for concomitant pathology of digestive system in HIV-infected patients. The role of GPs in monitoring cases of pathology of the digestive system of HIV-infected patients was quite low. 61.3% of specialty physicians were also unable to answer about the route of the HIV-infected person.
- The low level of awareness of the interviewed GPs and specialty physicians on the control of treatment of digestive system pathology, algorithms of action and routes of HIV-infected patients with comorbid digestive system pathology was revealed.
- The frequency of counter-referrals by specialty physicians of patients to GPs for concomitant pathology, including organs of the digestive system, was quite low, both according to the answers of GPs and the answers of specialty physicians. Moreover, the return of such patients to GPs occurred mainly in the case of achieving a stable virological response, and only occasionally during ART in the event of exacerbation of somatic diseases, in connection with the manifestation of digestive system pathology, which could actually lead to interruptions in ART. That is, patients who underwent ART and reacted negatively to it, almost did not return to GPs and therefore did not receive continued comprehensive and coordinated medical care for various pathologies of the digestive system. That is, the return of HIV-infected patients from specialty physicians to GPs was low, episodic, which may explain the decline in the ability of GPs to effectively monitor the clinical outcome of treatment of digestive system pathology and side effects of ART in HIV-infected patients.
- Certain problems were identified in the detection of digestive system pathology in HIV-infected people and the subsequent management of such patients. Determined certain inconsistencies and insufficient screening of comorbid pathology of the organs of the digestive system in HIV-infected patients in the practice of GPs may mean that many chronic pathologies remain undetected. The untreated comorbid diseases of the digestive system in HIV infection may be a risk factor for reduced ART efficacy in such patients. In this regard, special attention of primary care physicians, especially family physicians, should be paid to the timely detection, treatment and monitoring of digestive system diseases in HIV-infected patients.
- It seems appropriate to clarify the roles and implement clear algorithms for joint action of GPs and specialists involved in the management of HIV-infected patients with concomitant digestive system pathology, as physicians' opinions sometimes differed markedly even within each of the three occupational groups of respondents. The need to raise the awareness of GPs and specialty physicians about effective strategies and optimization of their current practice on screening and current approaches to the management of HIV-infected patients with concomitant pathology of the digestive system has been identified.
Association with scientific programs and funding
The study is a fragment of the research work of NMU named after O.O. Bogomolets "Development of a system to counter the spread of socially dangerous bloodborne viral infections at the level of primary health care in the context of public health in Ukraine", funding from the Ministry of Health of Ukraine from the State Budget of Ukraine (state registration № 0118U001212).
References
- HIV/AIDS surveillance in Europe 2019 – 2018 data. HIV/AIDS surveillance in Europe 2019 – 2018 data. https://www.ecdc.europa.eu/sites/default/files/documents/hiv-surveillance-report-2019.pdf.
- Nakaz MOZ Ukrainy vid 05.06.2019 № 1292 Pro zatverdzhennia novoho Klinichnoho protokolu iz zastosuvannia antyretrovirusnykh preparativ dlia likuvannia ta profilaktyky VIL-infektsii. http://moz.gov.ua/article/ministry-mandates/nakaz-moz-ukraini-vid-05062019--1292-pro-zatverdzhennja-novogo-klinichnogo-protokolu-iz-zastosuvannja-antiretrovirusnih-preparativ-dlja-likuvannja-ta-profilaktiki-vil-infekcii.
- HIV Infection in Ukraine. Informatsiynuy Buleten. 2020;(51). https://phc.org.ua/sites/default/files/users/user90/HIV_in_UA_51_2020.pdf.
- Samji H, Cescon A, Hogg RS, Modur SP, Althoff KN, Buchacz K, Burchell AN, Cohen M, Gebo KA, Gill MJ, Justice A, Kirk G, Klein MB, Korthuis PT, Martin J, Napravnik S, Rourke SB, Sterling TR, Silverberg MJ, Deeks S, Jacobson LP, Bosch RJ, Kitahata MM, Goedert JJ, Moore R, Gange SJ. Closing the Gap: Increases in Life Expectancy among Treated HIV-Positive Individuals in the United States and Canada. Okulicz JF, ред. PLoS ONE. 2013;8(12). doi:https://doi.org/10.1371/journal.pone.0081355
- Neuhaus J, Angus B, Kowalska JD, Rosa A, Sampson J, Wentworth D, Mocroft A. Risk of all-cause mortality associated with nonfatal AIDS and serious non-AIDS events among adults infected with HIV. AIDS. 2010;24(5). doi:https://doi.org/10.1097/QAD.0b013e3283365356
- Akhmedzhanova Z, Urunova D, Isaeva G. Rasprostranennost i chastota soputstvuyuschih i opportunisticheskih zabolevaniy na raznyih stadiyah VICh-infektsii. Zhurn. teoretich. i klin. Meditsinyi. 2015;4.
- Piroth L. Liver steatosis in HIV-infected patients. Aids Reviews. 2005;7(4).
- Alekseeva A, Nguen I, U K. Dynamika vyiavlennia deiakykh suputnikh patolohii ta staniv u osib z vpershe vstanovlenym diahnozom VIL-infektsii v Ukraini. Profilaktychna medytsyna. 2016;26(1).
- Hetman L, Voronova K, Riabinchuk M. Otsinka klinichnykh kompetentsii medychnykh pratsivnykiv zakladiv okhorony zdorovia, shcho nadaiut antyretrovirusnu terapiiu. Profilaktychna medytsyna. 2016;26(1).
- Nakaz MOZ Ukrainy vid 05.08.2014 № 509 Pro zatverdzhennia Zmin do Typovoho polozhennia pro kabinet "Dovira". Published online 2014.
- Golubovskaya О. Problemyi okazaniya meditsinskoy pomoschi bolnyim VICh-infektsiey i virusnyimi gepatitami v Ukraine. Klinicheskaya infektologiya i parazitologiya. 2013;(4).
- Vysotska O, Holubovska O. Aktualni pytannia protydii poshyrenniu sotsialno-nebezpechnykh hemokontaktnykh virusnykh infektsii v suchasnii systemi hromadskoho zdorovia Ukrainy: rol pervynnoi medychnoi dopomohy. Ukraina. Zdorovia natsii. 2018;(3).
- Landon BE. Physician Specialization and the Quality of Care for Human Immunodeficiency Virus Infection. Archives of Internal Medicine. 2005;165(10). doi:https://doi.org/10.1001/archinte.165.10.1133
- Nanditha NGA, St-Jean M, Tafessu H, Guillemi SA, Hull MW, Lu M, Henry B, Barrios R, Montaner JSG, Lima VD. Missed opportunities for earlier diagnosis of HIV in British Columbia, Canada: A retrospective cohort study. Sued O, ред. PLOS ONE. 2019;14(3). doi:https://doi.org/10.1371/journal.pone.0214012
- Rogowska-Szadkowska D, Strumiło J, Chlabicz S. Knowledge of family medicine trainers concerning HIV/AIDS – pilot study. Przeglad epidemiologiczny. 2017;71(4).
- Traversy G, Austin T, Yau J, Timmerman K. Assessing uptake of national HIV screening and testing guidance—Part 1: Awareness, use and usefulness. Canada Communicable Disease Report. 2017;43(12). doi:https://doi.org/10.14745/ccdr.v43i12a03